Fill Your Cna Shower Sheets Form
Different PDF Templates
Hazmat Shipping Papers Template - Federal and state regulations must be followed throughout the shipping process.
For further assistance and to ensure you have a complete understanding of this important legal document, you can visit pdftemplates.info, which provides valuable information and resources regarding the California Power of Attorney form.
Free Printable Puppy Health Guarantee Template - The contract details the responsibilities of both the Buyer and Breeder.
Similar forms
The CNA Shower Sheets form serves a critical function in monitoring the skin health of residents during showering. It is similar to the Patient Assessment Form, which also emphasizes the importance of visual assessments. Both documents require caregivers to evaluate the physical condition of patients, documenting any abnormalities. The Patient Assessment Form, like the CNA Shower Sheets, includes sections for specific findings, allowing healthcare providers to communicate effectively about a patient’s status.
Another document akin to the CNA Shower Sheets is the Incident Report Form. This form is used to document any unusual occurrences or accidents involving residents. Both documents prioritize the immediate reporting of issues to higher authorities, such as charge nurses or directors of nursing. The Incident Report Form focuses on events that may lead to injury, while the CNA Shower Sheets specifically targets skin conditions, but both serve to enhance patient safety and care quality.
The Skin Assessment Tool is also comparable to the CNA Shower Sheets. This tool is designed to monitor skin integrity and identify risks for pressure ulcers. Both forms require detailed observations and descriptions of skin conditions. The Skin Assessment Tool may include a scoring system to quantify risk, while the CNA Shower Sheets focus more on specific abnormalities observed during showers, yet both aim to ensure proactive care for residents.
The Daily Care Log is another document that shares similarities with the CNA Shower Sheets. Caregivers use this log to record daily activities and observations about residents. Like the CNA Shower Sheets, it emphasizes the importance of documenting care provided and any changes in a resident's condition. Both forms facilitate communication among the care team, ensuring that all members are informed about the resident's health status.
The Nursing Progress Notes are also relevant to the discussion. These notes are used by nurses to document ongoing assessments and interventions for residents. Similar to the CNA Shower Sheets, they require clear descriptions of findings and actions taken. Both documents serve to create a comprehensive record of care, enhancing the continuity and quality of treatment for residents.
The Care Plan is another document that aligns with the CNA Shower Sheets. This plan outlines the specific needs and goals for a resident’s care. Both documents require input from caregivers and aim to address any identified issues. While the Care Plan focuses on long-term strategies, the CNA Shower Sheets provide immediate observations that can influence adjustments to the care plan.
The Medication Administration Record (MAR) is also similar to the CNA Shower Sheets. The MAR tracks medications given to residents, including any reactions or side effects. Both documents require attention to detail and prompt reporting of any adverse findings. The CNA Shower Sheets focus on skin conditions, while the MAR focuses on medication effects, but both are crucial for ensuring resident safety and well-being.
The Fall Risk Assessment Form is another document that shares commonalities with the CNA Shower Sheets. This form evaluates a resident's risk of falling, requiring detailed observations and assessments. Both documents aim to identify potential hazards to residents' health. While the Fall Risk Assessment focuses on mobility and environmental factors, the CNA Shower Sheets emphasize skin integrity, yet both play a vital role in comprehensive resident care.
For those looking to formalize the sale of an item, it is essential to have a Bill of Sale that captures both the details of the transaction and the agreement between seller and buyer. This document helps to protect both parties and serves as a reference for future disputes. Individuals may find it useful to access a template for the document, ensuring all necessary information is accurately recorded.
Lastly, the Infection Control Checklist is comparable to the CNA Shower Sheets. This checklist is used to monitor practices that prevent infections within healthcare settings. Both documents require diligent observation and reporting of any issues that could affect a resident’s health. While the Infection Control Checklist targets infection prevention, the CNA Shower Sheets focus on skin conditions, yet both contribute to the overall safety and health of residents.
Instructions on Writing Cna Shower Sheets
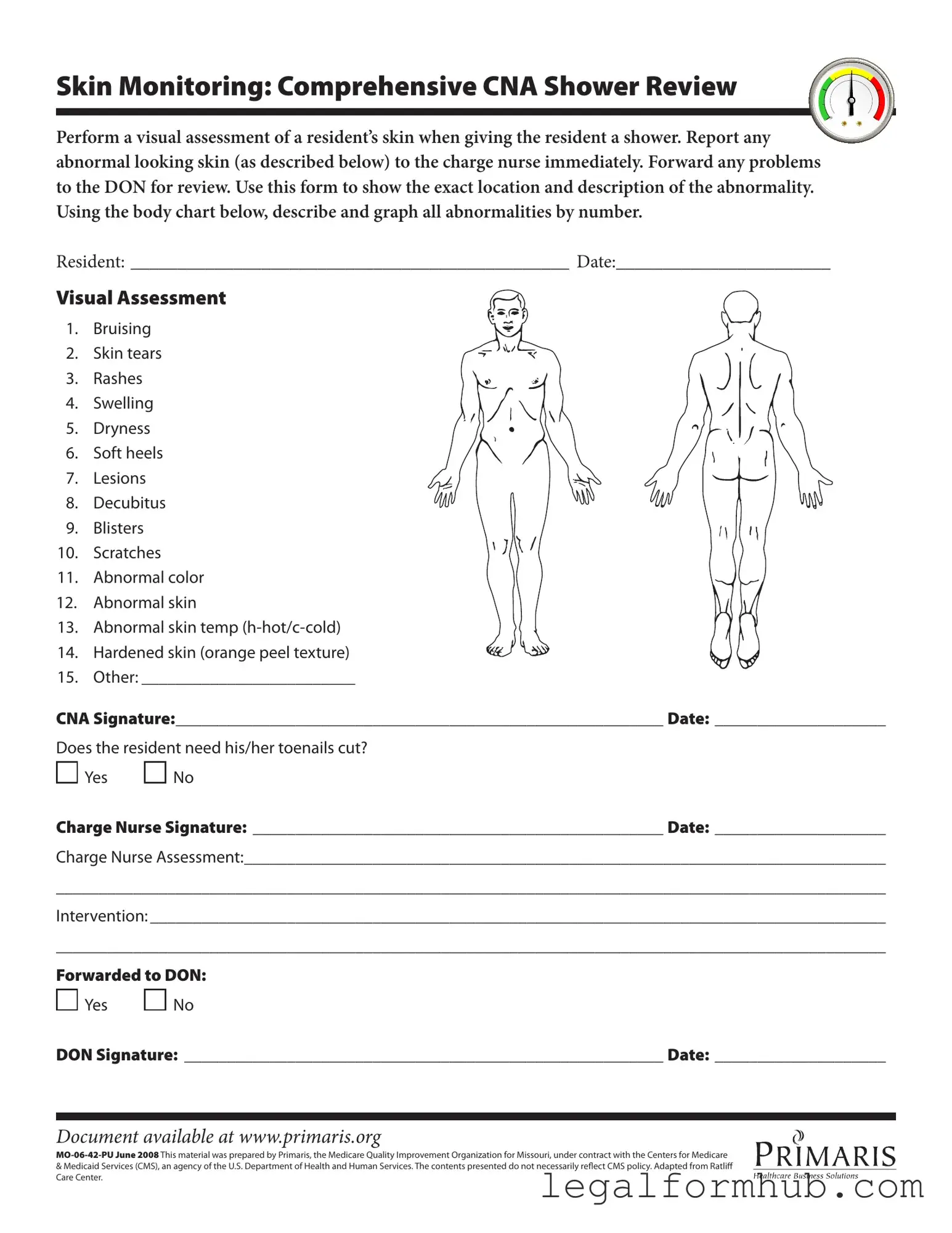
Filling out the CNA Shower Sheets form is essential for documenting skin assessments during resident showers. This ensures that any abnormalities are reported and addressed promptly. Follow these steps to complete the form accurately.
- Begin by entering the resident's name in the designated space labeled RESIDENT:.
- Fill in the date of the assessment next to DATE:.
- Conduct a visual assessment of the resident's skin while showering. Look for any abnormalities such as bruising, skin tears, or rashes.
- Use the body chart provided on the form to indicate the location of any abnormalities. Number each abnormality according to the list provided.
- In the section for visual assessment, check off any abnormalities you observe, including:
- Bruising
- Skin tears
- Rashes
- Swelling
- Dryness
- Soft heels
- Lesions
- Decubitus
- Blisters
- Scratches
- Abnormal color
- Abnormal skin
- Abnormal skin temperature (hot or cold)
- Hardened skin (orange peel texture)
- Other: _________________________
- Sign the form in the space provided for CNA Signature: and date it.
- Indicate whether the resident needs their toenails cut by checking either Yes or No.
- Have the charge nurse sign the form in the space labeled Charge Nurse Signature: and provide the date.
- In the Charge Nurse Assessment: section, document any observations or concerns regarding the resident's skin condition.
- For the Intervention: section, outline any actions taken or recommended based on the assessment.
- Indicate whether the report has been forwarded to the Director of Nursing (DON) by checking Yes or No.
- Finally, the DON should sign the form in the space provided and include the date.
Misconceptions
Misconceptions about the CNA Shower Sheets form can lead to misunderstandings regarding its purpose and use. Here are four common misconceptions:
- It is only for documenting serious skin issues. Many believe that the form is only necessary when there are severe skin problems. In reality, it is important to document all skin assessments, including minor issues, to ensure comprehensive care.
- Only the CNA needs to fill it out. Some assume that only the Certified Nursing Assistant (CNA) is responsible for the form. However, collaboration with the charge nurse and the Director of Nursing (DON) is essential for proper follow-up and intervention.
- Skin assessments are optional during showers. There is a misconception that skin assessments can be skipped if time is short. This is not true. Regular assessments are crucial for identifying and addressing potential skin issues early.
- The form is not necessary if no abnormalities are found. Some think that if no abnormalities are noted, the form does not need to be used. This is incorrect. Documenting the assessment, even when everything appears normal, is vital for maintaining accurate health records.
Key takeaways
Filling out and using the CNA Shower Sheets form effectively is crucial for monitoring resident skin health. Here are key takeaways to keep in mind:
- Visual Assessment: Conduct a thorough visual assessment of the resident's skin during the shower. This includes checking for bruises, rashes, and other abnormalities.
- Documentation: Clearly document any findings on the form. Use the body chart to indicate the exact location and description of any skin issues.
- Immediate Reporting: Report any abnormal findings to the charge nurse right away. Timely communication is essential for resident care.
- Follow-Up: Ensure that any problems are forwarded to the Director of Nursing (DON) for further review and intervention.
- Nail Care: Note whether the resident needs toenail care. This is an important aspect of overall skin health and hygiene.
By following these guidelines, you can help ensure that residents receive the necessary attention for their skin health during showering.
File Information
| Fact Name | Details |
|---|---|
| Purpose | The CNA Shower Sheets form is designed for documenting skin assessments during resident showers. |
| Visual Assessment | It includes a comprehensive visual assessment of the resident's skin, focusing on abnormalities. |
| Abnormalities List | The form lists 15 potential skin issues, such as bruising, rashes, and decubitus. |
| Reporting Protocol | Any abnormalities must be reported to the charge nurse immediately for further action. |
| Documentation Requirement | It requires specific documentation of the exact location and description of any skin abnormalities. |
| Signature Requirement | Both the CNA and the charge nurse must sign the form to confirm the assessment and actions taken. |
| Forwarding Process | Abnormalities may be forwarded to the Director of Nursing (DON) for further review and intervention. |
| State-Specific Law | This form is governed by Missouri state regulations regarding nursing home care and resident safety. |
| Resource Availability | The document is available online at www.primaris.org for reference and training purposes. |